
Surgery Residency
General Surgery Residency - Experience
1. Dr. Maria, a graduate of a “hybrid” surgical residency program on the east coast.
While many other mundane details have faded, I distinctly remember my very first day as a PGY1 (post-graduate year 1), aka “intern” in my surgical residency. I was, in my long white coat, doctorly, pockets overburdened with heavy reference manuals for diseases, one for medications, a notepad, pens, a stethoscope, my smartphone with the latest medical apps, much like a school-aged kid with freshly sharpened pencils, having absolutely No Idea what was to come.
But I do recall, having been left with other interns post-rounds to write orders, and, gulp, dictate discharge summaries, thinking that this was the greatest job ever.
Now, I would be pulling the wool if I attested here that this was my prevailing overriding sentiment of a general surgery residency. But, the immersion, the learning, exposure, not only to surgical concepts and skills, but to the inner workings of medicine itself, the dynamic of a tertiary care center and its ready-made collaborative environment and learning about interactions with persons in their most vulnerable, at times, most tragic circumstances, that value is incalculable.
I had matriculated into medical school determined to go into emergency medicine, but it was an amazing surgery rotation during third year that convinced me to instead apply into general surgery- I am not great at prolonged sitting or prolonged, exhaustive, 50-problem list-style rounding, but I also relished delving into subject matter, getting into the guts of things, so to speak. Well, it doesn’t get more gut-filled than general surgery- this discipline is a great amalgam of thinking and doing, and, importantly, learning when NOT to do.
While, as moderated through the ACGME, there are baseline requirements for surgical residencies, such as case numbers in each category, as in any specialty, residency experiences vary tremendously depending on the nature of the institution, the affiliated staff and the surrounding environment. Academic centers will by default be more research-immersed, and generally have more built- in layers between the resident and the attending, whereas community-based programs may lend to more informal flow and interactive experience but may not provide level of specialization or formalized didactics. That is not to say, however, that you will not be taught by extremely skilled and astute surgeons and other staff in a community setting. If you relish a more traditional environment, do consider the lauded academic institutions, but if you instead prefer a more relaxed paradigm, and consider yourself self-motivated, then you may be more suited to community-based program.
Do also consider the availability of subspecialists in your hospital, such as, for example, urology, neurosurgery, cardiothoracic surgery, plastics, etc, as their installment may provide for rotations as well as informal learning- if they are there, you will get to know them, and you will find yourself working with them not rarely. Likewise, learn about the number of fellows you may expect to work with, for; fellows may relegate the resident to a lesser role in a procedure.
Expect time served in surgical intensive care, minor procedure room, general/acute care surgery, vascular surgery, pediatric surgery, minimally invasive (laparoscopic/robotic) surgery, perchance bariatric surgery, surgical oncology, endoscopy, trauma surgery, as well as off-service opportunities such as cardiothoracic, ObGyn, research, etc.
You will round early, quite early, each morning, in order to complete assessments and plans prior to the start of the OR, and will often round later in the afternoon. There will typically be one morning per week dedicated to conferences and M&M (you will present).
I matched into what is considered more of a hybrid program- e.g. within a tertiary care center but without an associated medical school or fellows; really, it was the best of both worlds, as we had the exposure to level I trauma and all of the associated subspecialities, but also had more immediate contact with attendings. Our vascular numbers were significantly greater than most other programs, due to high-level vascular surgery and the absence of fellows. We operated a lot.
Now, we are in a new era with respect to residency. No longer can you toil until you are asleep on your feet- work is, at least officially, often apportioned into bite-sized aliquots as opposed to the week-long hospital stays of yore, which lends itself certainly to greater work-residency balance, but also may detract just a bit from continuity of care. That being said, show up early, stay late, get ‘er done and take ownership of the patient.
Overall, it is a bittersweet combination of incredible alliances and friendships, unbounded mental and physical and emotional fatigue, paralyzing self-doubt, punctuated by moments of triumph and clarity. I will never, ever, forget the call-room shenanigans (creating silly shorts from old scrubs, watching the Llama Song on repeat, taking advantage of someone’s open Netflix account to pepper their preferences with tacky movies), but also the somber moments that stretched into eternity, the throwing an emergent OR into play even though survival changes were slim, watching firsthand as an ICU patient’s support requirements kept escalating in spite of everything, climbing in conjunction with their lactate, releasing their abdominal sutures as one final hail Mary that perhaps it was all compartment syndrome (it wasn’t), seeing that TBI child, months later, who was ever teetering between life and death, come back to visit with their beaming parent, setting up an impromptu OR in the NICU at 2 AM for that infant with necrotizing enterocolitis found to have completely dead small bowel, sewing up that tiny abdomen to return to the parents, celebrating a successful transplant with an over-crowded hospital room of grateful family.
It's all there.
As to what comes after, you are, after completion of your surgical residency, free to chart your course, be it a fellowship or practice, and there is also a rising need for the surgicalist, surgery’s counterpart to the hospitalist. You will be in need, regardless of your destination.
A word of caution, particularly if your intent is to head directly into practice- you must advocate for yourself during training and ensure that you are learning what you need to practice independently.
Enjoy the journey.
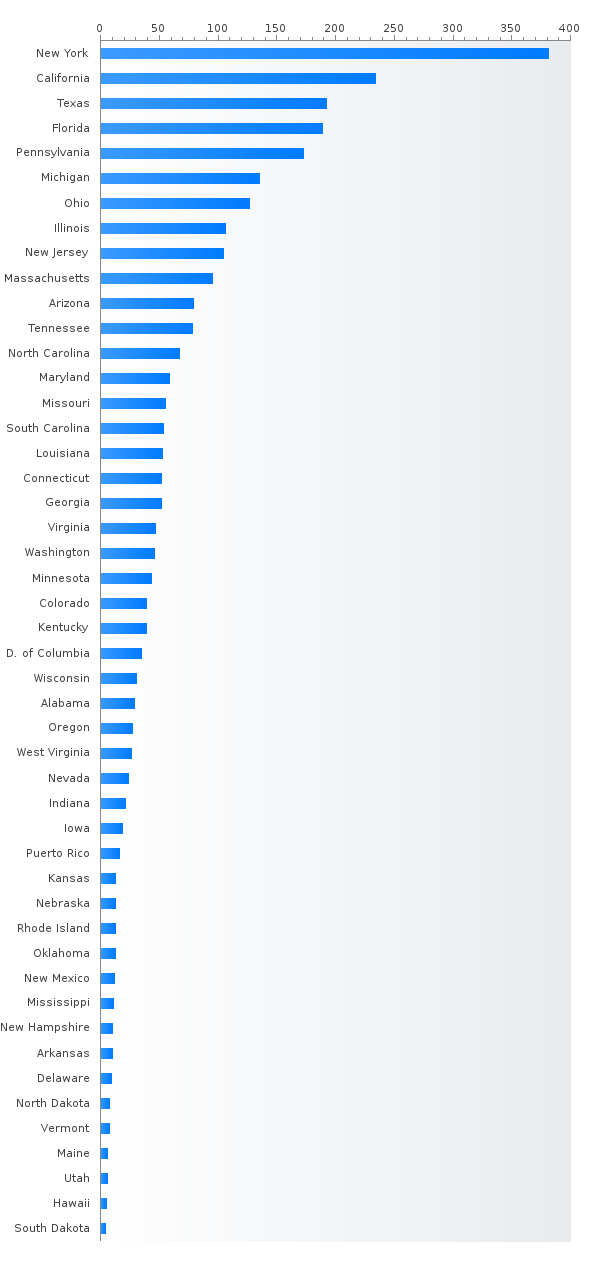
Read morePGY-1 Surgery residency positions by state
- New York (391)
- California (248)
- Florida (224)
- Texas (213)
- Pennsylvania (174)
- Michigan (136)
- Ohio (135)
- Illinois (114)
- New Jersey (108)
- Massachusetts (96)
- Tennessee (80)
- Arizona (78)
- North Carolina (76)
- Maryland (58)
- Georgia (57)
- South Carolina (56)
- Louisiana (55)
- Virginia (52)
- Missouri (52)
- Connecticut (48)
- Washington (45)
- Minnesota (41)
- Colorado (39)
- Kentucky (38)
- District of Columbia (35)
- Wisconsin (33)
- Alabama (32)
- Oregon (28)
- West Virginia (27)
- Nevada (24)
- Puerto Rico (23)
- Kansas (22)
- Indiana (21)
- Iowa (20)
- Oklahoma (18)
- Nebraska (13)
- Rhode Island (13)
- New Mexico (11)
- New Hampshire (11)
- Delaware (10)
- Arkansas (10)
- North Dakota (9)
- Mississippi (9)
- Utah (8)
- Vermont (8)
- Maine (6)
- Hawaii (5)
- South Dakota (4)
Most competitive Surgery residencies - Top 20 ranking
Top 10 most competitive Surgery residencies with %DO > 25
Percent MD,DO,IMG Surgery PGY-1 residents (main match)
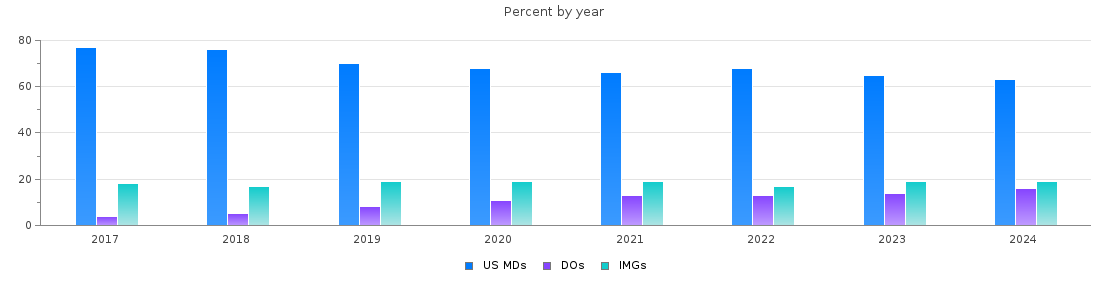
Surgery PGY-1 main residency Match statistics
| Year | Positions | Filled(%) | MD | DO | IMGs |
| 2026 | 3014 | 81.9 | 1554 (51 %) | 411 (13 %) | 503 (16 %) |
| 2025 | 2972 | 82.3 | 1539 (51 %) | 365 (12 %) | 542 (18 %) |
| 2024 | 2869 | 80.7 | 1474 (51 %) | 382 (13 %) | 458 (15 %) |
| 2023 | 2803 | 80.2 | 1483 (52 %) | 333 (11 %) | 431 (15 %) |
| 2022 | 2772 | 81.2 | 1545 (55 %) | 308 (11 %) | 396 (14 %) |
| 2021 | 2705 | 80.4 | 1451 (53 %) | 299 (11 %) | 425 (15 %) |
| 2020 | 2710 | 78.0 | 1443 (53 %) | 251 (9 %) | 420 (15 %) |
| 2019 | 2555 | 77.6 | 1407 (55 %) | 178 (6 %) | 395 (15 %) |
| 2018 | 2682 | 82.1 | 1678 (62 %) | 127 (4 %) | 395 (14 %) |
| 2017 | 2606 | 80.3 | 1617 (62 %) | 93 (3 %) | 383 (14 %) |
General surgery residency in numbers
1807 categorical and 1207 preliminary PGY-1 general surgery residency positions offered. It is around 8% of all residency positions. 99.7% of categorical positions were filled during the main match. The match rate among interviewed candidates is around 70% for US MDs, 60% for DOs, and 29/21% for US/non-US IMGs. Only 54% of preliminary positions were filled during the main match while the rest of preliminary positions were filled during the SOAP. Leaving places for the SOAP (usually for partially matched or highly qualified unmatched candidates) is a common behavior for general surgery preliminary residency match. With 45-65% match rate among interviewed US MD candidates scored Step 2 230-240, general surgery is a competitive specialty even for US MDs.