
Internal medicine Residency
Internal Medicine Residency - Experience
1. Dr. Rebecca Smith, Internal medicine resident, categorical university-based program
**Ring, ring, ring. It’s still dark outside but another work day in residency begins.
I am a US MD medical school graduate who completed Internal Medicine residency in an academic program in the midwestern United States. I was subsequently asked to stay as a Chief Resident. Now I work in the field of hospital medicine where I teach residents on a regular basis.
Residency was a challenging an amazing time in my life. Most medical (as opposed to surgical) fellowships require the completion of an Internal Medicine residency. This was a big part of why I chose Internal Medicine as a field so that I could keep my future career options open.
Categorical internal medicine residency length in the US is 3 years. IM residency has to comply by a set of standards outlined by the ACGME organization. Each residency program is required to abide by these regulations to remain accredited. Consequently, there are some things that all residency programs have in common.
All medicine residencies require a mix of both inpatient and outpatient medical training. Most residencies require that residents have their own supervised clinic in which they care for patients on an ongoing basis through all three years of training. This was true of my residency. I had an afternoon clinic every Wednesday for all 3 years. The faculty supervision was the same attending physician this entire time. Though I did not end up doing a clinic based practice, I did really enjoy the clinic environment. The ongoing relationship with a consistent faculty member was a great experience. It allowed me to really get to know his practice style and he was an excellent mentor. It was also nice to develop a relationship with patients whom I began to see regularly.
Residencies also have a significant component of inpatient hospital care. I spent several months each year of residency rotating a general inpatient service. As an intern (first year), I had the responsibility of admitting and managing several new patients each day and following them throughout their hospital stay. After intern year the responsibilities shifted more to supervision of first year residents and medical students. All rotations were supervised by an attending physician. This was the part of medicine that was the most interesting to me and why I eventually decided to become a hospitalist.
Each year there are several months devoted to the medical specialties. I was assigned to rotations like pulmonology, cardiology, gastroenterology, nephrology, etc. These were usually a mix of both inpatient and outpatient experience. Another things that most residencies have in common is didactic teaching sessions. There is some variability in how these are implemented. In the program I attended there were 2 mandatory conferences each day which were called “morning report” and “noon conference.” The morning session was a case presentation which was presented by residents and faculty present would quiz residents in the room about how they would choose to evaluate the patient. The noon conference was a lecture given by rotating medical faculty. There were also some special conferences like tumor board, morbidity and mortality conference, a rotating CME conference for the faculty, etc.
Residency rules limit the number of patients that a resident can care for. The rules also regulate how many duty hours can be worked and the supervision level required. Each residency will vary in respect to how these rules are implemented. Some programs use a call system overnight in which the residents rotate staying overnight to care for the patients. Other programs use a system of dedicated overnight rotations (usually called night float) to care for patients. My program did the former.
There were a few things I was unprepared for when I started residency. As alluded to above, the diminished amount of time that I could devote to self care should not have surprised me since I already knew about the residency work hours but when residency began I really struggled finding the time to do these things. Another thing I was unprepared for is how many times I was called for the nursing staff for relatively small problems but didn’t really know what to do. It took me a few months to memorize the common medications and doses used for these routine problems. As a medical student, I always had time to look up medications and doses since I wasn’t the one being called first. Needing to come up with an answer without being given much time to think about it was hard for me at first.
I was asked and chose to do a 4th year called a “chief resident” year. This was primarily an administrative year. I learned to manage the residents, made the schedules, interviewed new applicants, and served as an intermediary between residents and faculty when needed. I chose to do this year both because it was an honor to be asked and also because it allowed me some additional time to decide if I wanted to do a medical fellowship.
Residency was a period of tremendous growth and learning for me. My medical knowledge skyrocketed and my confidence improves as well. I also made some great friendships with the other residents since we worked so closely together. There are also challenges in residency. The work hours are very long and the work is a huge responsibility which caused me a lot of fatigue, both physical and mental. The long, irregular hours also made it difficult to coordinate non-work responsibilities. Things like personal health care, dental visits, grocery shopping, cleaning, etc were often difficult to manage.
I now work in a more community based program (compared to the academic environment I trained in). There do seem to be some differences. The teaching and didactic programs at my community program are all geared toward resident teaching. I don’t think the residents here really get any exposure to faculty level teaching and CME. The amount of faculty oversight seems to be higher at this community program than where I trained. The academic residency was at a much larger institution which required residents to keep running. Community programs are set up to run with private practice physicians and residents are just kind of added in. Consequently, I’m not sure the expectations for residents are quite as high in the community program as there were in a more academic setting. However, it also seems like a much kinder environment where residents can take a little more time to learn at their own pace rather than the frantic quick paced program where I trained.
Overall, I really enjoyed the residency experience and am grateful for the opportunity to have become an Internal Medicine physician.
2. Dr. Yasmin, graduate of preliminary Internal Medicine internship at University of California San Diego
Many specialties (such as Neurology, Radiology, Dermatology, Ophthalmology) require a preliminary internship in Internal Medicine. As a neurology resident, I chose a program that was the best fit for me, and I will explain why.
First, internal medicine internship at a major academic hospital is a challenging, life-changing time full of personal and academic growth. There are various internships you can find throughout the country; some are less intense than others in terms of the volume and complexity of patients and balance of inpatient vs outpatient time. My advice to applicants would be, if you are entering a specialty that is heavily reliant on medical issues (such as neurology, dermatology) and wish to be the best in your residency, do not pick an “easier” program just to save you some stress in intern year. The more you learn and the more experience you get with challenging cases, the smarter and more prepared you will be in your advanced residency program. I say this now, as a PGY-4 neurology resident, that I have to routinely manage cardiac, pulmonary, infectious, hematologic, and renal issues in my neurology inpatients. While we do of course rely on consultants in these fields, it is of paramount importance to recognize and manage basic medical issues as the primary team. A solid internal medicine program will prepare you best for this. My preliminary year was treated no differently to the other categorical internal medicine residents, with the exception that I had no continuity clinic.
Internal medicine preliminary years will have a variety of balance between inpatient time and outpatient time, critical care time and general medicine wards time. The particular mix will vary for each resident. I personally had about 3 months of critical care ICU team (divided into medical ICU, cardiac ICU, and the general ICU at the VA hospital affiliated with UC San Diego). This was an overwhelming experience for an intern, who is just getting used to putting in orders, working with nurses, and learning medicine while managing critically ill patients. It was, however, a very important part of my medical knowledge. The balance between ICU rotations and general ward rotations is something to ask about when looking for preliminary programs. Again, if your destination specialty is something that will be inpatient heavy (such as, neurocritical care) then having more ICU experience in your intern year is valuable.
The majority of my preliminary year was inpatient time, with a few blocks of interspersed specialty clinics. While this served to gain me heavy exposure to inpatient medicine, I did feel a lack of understanding of primary care issues in the outpatient setting. This is because my preliminary program did not have a continuity resident clinic for the preliminary interns. If longitudinal outpatient care is something you enjoy, then seeking a program with more clinic time is key. I personally will not be doing outpatient medicine in my future, so it was ok with me.
Inpatient medicine at my hospital was busy, with interns carrying 6-8 patients at my hospital. Our team structure is pretty standard; two interns, one senior resident, and one attending. We would round every day on up to 16 patients, and alternate admitting days between us. We have a mix of “bread and butter” diagnoses; COPD, heart failure, diabetes, cellulitis, osteomyelitis, HIV and AIDS associated complications, and we also had our fair share of “zebras” – lupus and autoimmune conditions, extra-pulmonary tuberculosis, and more. One thing to consider is the location of the hospital when choosing a program. County hospitals or “safety-net” hospitals which take care of the underserved population tend to have a different type of medicine than hospitals in more wealthy areas. I enjoyed working with the underserved population and learning the types of social challenges faced by patients without access to food, housing, insurance and financial resources. I also saw more of the effects of substance use, opportunistic infections, and infections associated with travel to Mexico such as tuberculosis because of the proximity to the USA-Mexico border.
To conclude, preliminary internship at a major academic hospital is a challenging year. It is full of long work hours, nearly 80-hour weeks, lots of inpatient time, and little elective time or time off. However, the skills I learned and medicine knowledge was essential to having a successful advanced residency in Neurology for me, and for my future career. For these reasons, it is important to pick a program that will prepare you the best academically, keeping in mind the balance of inpatient and outpatient rotations, patient population, and geographical considerations. My final piece of advice is make sure your program respects and treats preliminary interns just as categorical interns, which was fortunately a strength of my program at UC San Diego, to make sure you have the best educational experience working as part of a team.
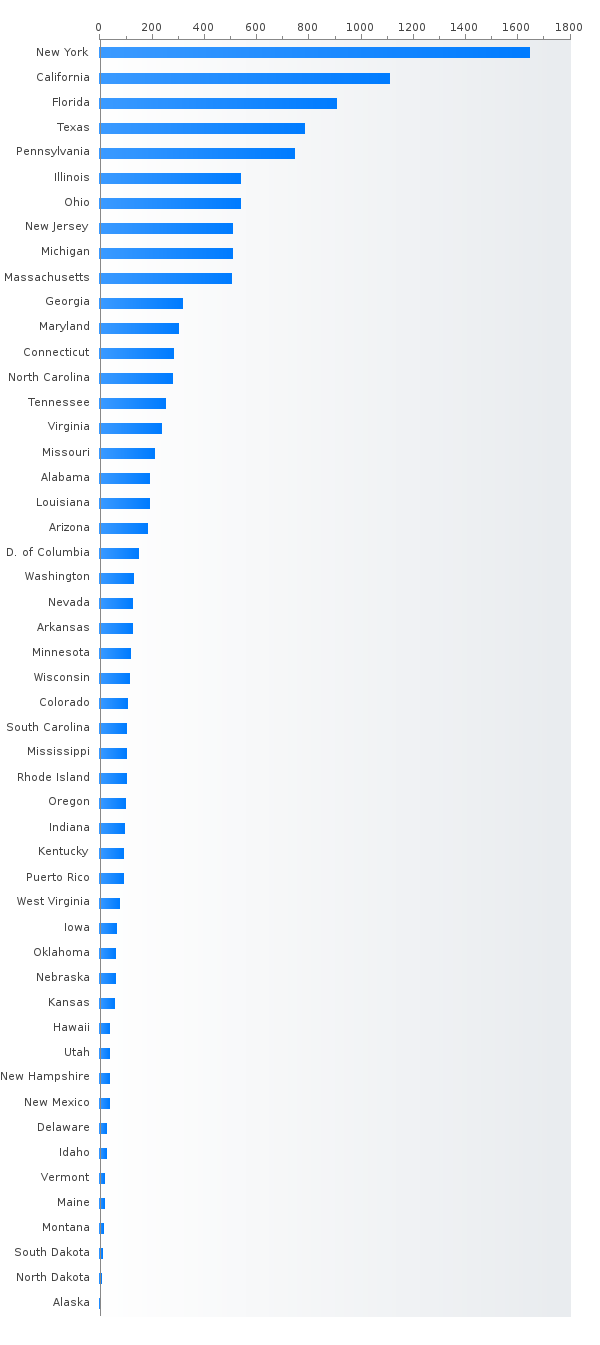
Read morePGY-1 Internal medicine residency positions by state
- New York (1750)
- California (1226)
- Florida (1035)
- Texas (878)
- Pennsylvania (737)
- Ohio (549)
- Illinois (539)
- New Jersey (534)
- Michigan (533)
- Massachusetts (502)
- Georgia (347)
- Maryland (296)
- Tennessee (284)
- Connecticut (282)
- North Carolina (279)
- Virginia (268)
- Arizona (232)
- Missouri (203)
- Louisiana (200)
- Alabama (191)
- District of Columbia (149)
- South Carolina (145)
- Washington (132)
- Wisconsin (131)
- Mississippi (127)
- Indiana (124)
- Arkansas (122)
- Nevada (121)
- Minnesota (120)
- Colorado (109)
- Kansas (105)
- Rhode Island (100)
- Oregon (100)
- Kentucky (95)
- Puerto Rico (90)
- Oklahoma (68)
- Iowa (62)
- Nebraska (59)
- Utah (44)
- New Mexico (38)
- New Hampshire (35)
- Hawaii (34)
- Delaware (31)
- Idaho (26)
- Montana (22)
- Vermont (18)
- Maine (17)
- North Dakota (12)
- South Dakota (9)
- Alaska (2)
Most competitive Internal medicine residencies - Top 20 ranking
Top 10 most competitive Internal Medicine residencies with %DO > 25
Percent MD,DO,IMG Internal medicine PGY-1 residents (main match)
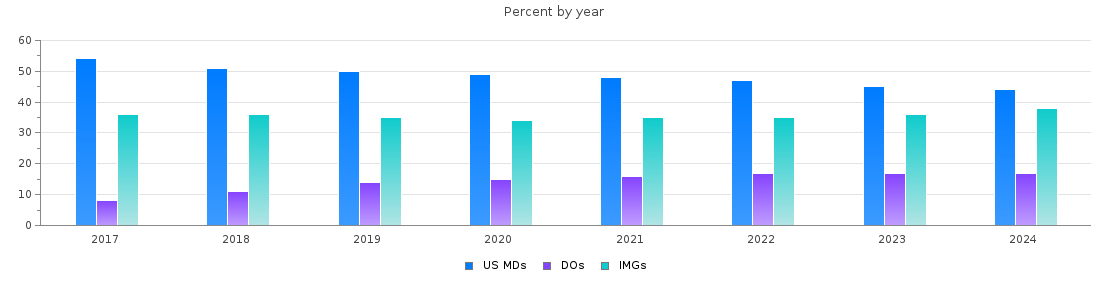
Internal medicine PGY-1 main residency Match statistics
| Year | Positions | Filled(%) | MD | DO | IMGs |
| 2026 | 13112 | 94.8 | 5525 (42 %) | 2121 (16 %) | 4782 (36 %) |
| 2025 | 12952 | 96.0 | 5299 (40 %) | 2122 (16 %) | 5015 (38 %) |
| 2024 | 12321 | 94.9 | 5163 (41 %) | 2010 (16 %) | 4516 (36 %) |
| 2023 | 11893 | 95.6 | 5210 (43 %) | 1956 (16 %) | 4196 (35 %) |
| 2022 | 11583 | 94.6 | 5182 (44 %) | 1878 (16 %) | 3898 (33 %) |
| 2021 | 11298 | 94.8 | 5158 (45 %) | 1763 (15 %) | 3784 (33 %) |
| 2020 | 11038 | 95.2 | 5218 (47 %) | 1658 (15 %) | 3628 (32 %) |
| 2019 | 10310 | 96.3 | 5026 (48 %) | 1396 (13 %) | 3502 (33 %) |
| 2018 | 9799 | 96.9 | 4925 (50 %) | 1065 (10 %) | 3505 (35 %) |
| 2017 | 9489 | 97.9 | 5069 (53 %) | 835 (8 %) | 3378 (35 %) |
IM residency is the top specialty in terms of the number of positions
Internal medicine offers around 11200 categorical, 1550 preliminary, and 440 primary care positions. The total number of positions increased by 33% over the past 10 years and currently about 700 ACGME accredited programs offer 32% of all available PGY-1 residency positions. The percentage of matched IMGs a bit increased over the past years while the percentage of US MDs a bit decreased. Scores below the average are still guarantee near 95% probability of the match for US MDs and DOs, while low scores for IMGs drastically reduce the probability of the match. 97% categorical and 89% preliminary internal medicine positions are filled during the main match. 25% of all matched US MDs, 25% of all matched DOs, and 48% of matched IMGs were matched into internal medicine residency positions. With the largest number of positions available internal medicine is the best application choice for many successful candidates.